
Proceeding of Early Intervention
- History Of IACP
- Constitution Of IACP
- Executive Members
- Membership
- Annual Conference
- Fellowship Opportunities
- IJCP Journal
- Research-Priorities
- CP Day Celebration Gallery
- Government Facilities
- Join Now
- Tutorials
- Family Forum
- Book Review
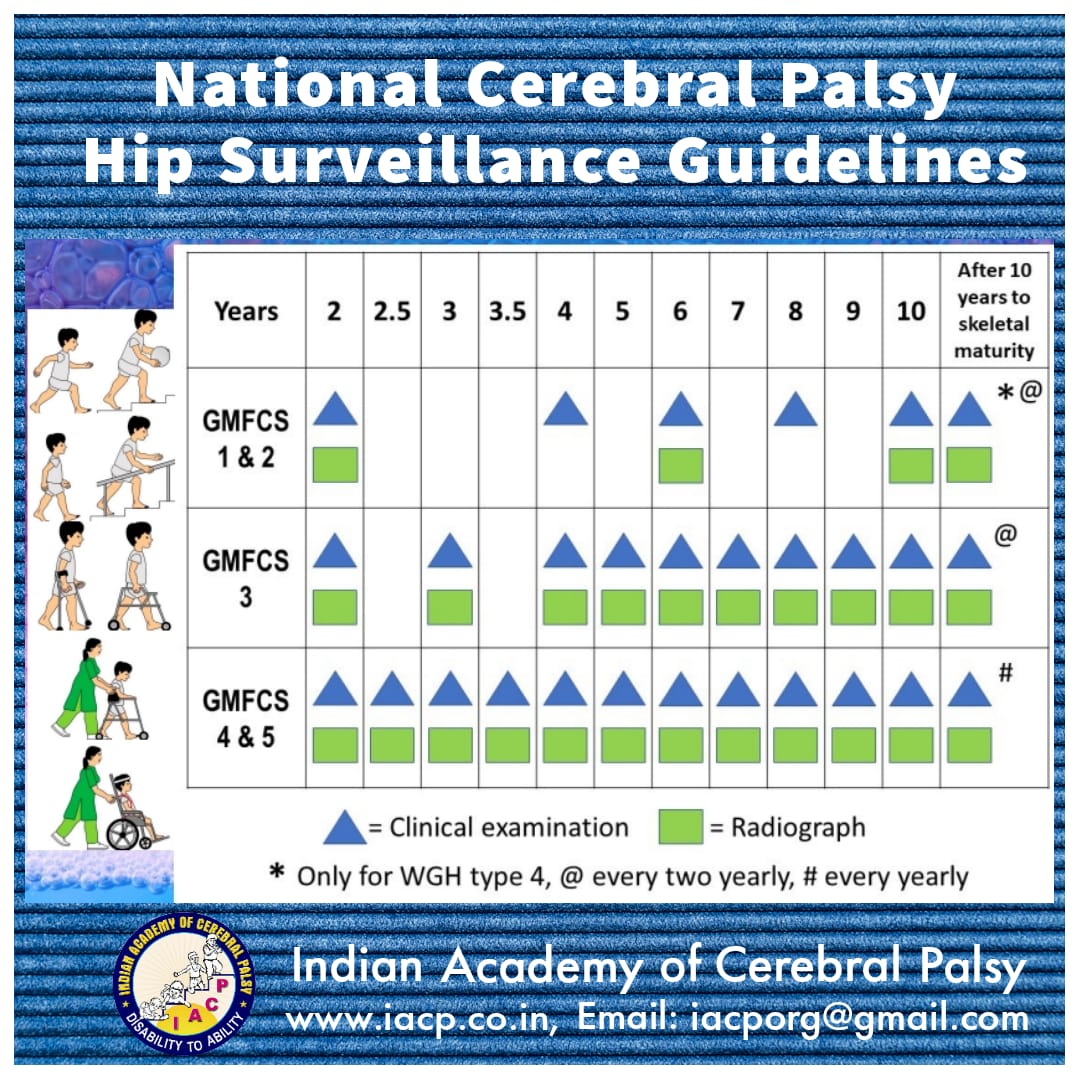
- National Cerebral Palsy Hip Surveillance Guidelines
- CP hip surveillance guidelines
- CP hip surveillance review
{kind=link}
22ND NOVEMBER 2008 12.-1.30 PM
Co-ordinator-
Dr.G. Shashikala
Participants:
Dr.Ashok Johari, Dr. Aniruddh Purohit, Dr. Pratibha singhi, Dr. Anaita Hegde, Dr. Medhini Padhye, Dr.Sanjay Wadhwa, Dr.Rabindran Issac, Mr. K.D. Mallikarjun JUDGES:- Prof. Peter Rosenbaum, Prof. M.S.Mahadeviah, Prof. Bhavana Lakkar, Dr. Sunanda Kolli.
Definition
AAMR definition – Provision of all those developmental services to the developmentally disabled child in the age group 0-6 years and his/ her family .so that he / she can compensate for the developmental lag.
2000 definition from Handbook of early childhood intervention edited by Shankoff JP, Meisels SJ[ special education perspective]
Early intervention consists of multidisciplinary services provided to children from birth to 5years of age to promote child health and well-being, enhance emerging competencies, minimize developmental delays, remediate existing or emerging disabilities, prevent functional deterioration, promote adaptive parenting and over all family functioning. These goals are accomplished by individualized developmental, educational and therapeutic services for children provided in conjunction with mutually planned support for their families.
- Do you agree with this definition? If yes, why? If no, why?
- Is this an adequate definition or is this a vague umbrella term?
- How will you interpret early-early in life or as early in the expression of the condition?
- What are advantages and disadvantages of both?
- Do you agree with the age group mentioned?
- What spectrum of dev. disorders should be covered?
- What should be the content of EI programs?
- What is the scientific rationale?
- What are the models of EI programs?
- What is suitable in Indian conditions?
- Who should be the leader of early intervention team and how do we build them?
- Is main streaming the beginning or end point of early intervention ?
- What should parents bring to early intervention ?
- Parent – Professional partnership – are they feasible in Indian context ?
- Family centered service – possibility or an ideal?
- How effective are early intervention programs?
- What is the evidence and how do we measure it?
- Are there any limitations?
- Are they cost effective?
- What is the reality as on today?
- Early intervention and rehabilitation-should we merge or differentiate?
- What should we do to implement EI programs successfully?
- What are your suggestions for advocacy?
Summary
Participants agreed with the second definition, felt it was a comprehensive & adequate definition but just too long to remember. It was also suggested that demands of society, participation & accent on child’s ability as the determining factor be added to this definition. Early was opined as -as early as diagnosis is possible. Suggestion of even intrauterine diagnosis was made. Caution in over diagnosing under the term high risk infants & avoiding too early labeling of disabilities was also stressed. Importance of developmental surveillance & monitoring was also stressed to avoid undue burden on early intervention services & unwanted anxiety to families. Age group up to 5 years was considered adequate & an index of suspicion for early picking of other developmental problems in the evolution of static encephalopathy in to developmental disability spectrum disorders were recommended.
Content of early intervention programs need to be global apart from accent on syndrome specific developmental domains starting from NICU care programs after detailed assessment Models in & around family need to be incorporated along with proper accent on cultural relevance & cost factor No method in particular has been proved more effective & there is a great need for programs to concentrate on improving family compliance with ample opportunities for activities & participation. Family centered model is a realistic & possible model for Indian conditions.
There was no agreement on who should be the leader in E.I. programs – it continues to be debate worthy point for future also. Parents need to bring more open information about the family itself & the performance of the child when he/she is not being supervised. Rehab measures should continue after 6 years under a different name-Life span care possibly.
Limitations are mainly due to lack of awareness & inadequate no of well trained professionals. Early intervention should be thought of both from the perspective of bio clinicians & community setting.
A few more questions were not discussed for lack of time. We intend to continue the debate till we evolve an acceptable model with most questions satisfactorily answered
We therefore request all members to mail their opinions to shashi_kola @ rediffmail.com for compilation to help complete the debate & have a consensus report.
Dr.G.Shashikala. Co ordinator