
Non Motor Gains of Botox
- History Of IACP
- Constitution Of IACP
- Executive Members
- Membership
- Annual Conference
- Fellowship Opportunities
- IJCP Journal
- Research-Priorities
- CP Day Celebration Gallery
- Government Facilities
- Join Now
- Tutorials
- Family Forum
- Book Review
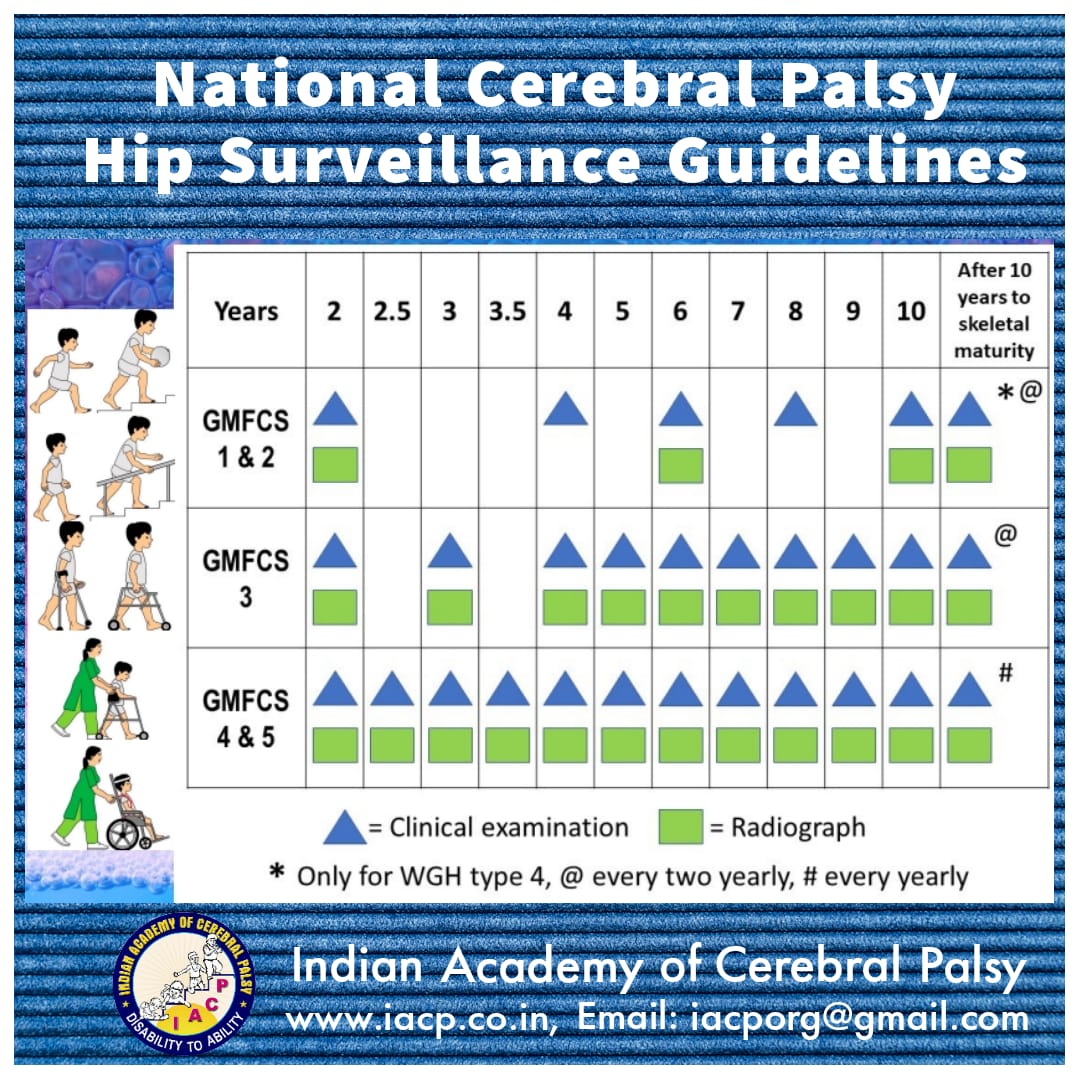
- National Cerebral Palsy Hip Surveillance Guidelines
- CP hip surveillance guidelines
- CP hip surveillance review
{kind=link}
Dr. Mrs. G. Shashikala, Ms. Pranali Somkuwar, Ms Vandana Giri & Mrs. Ujwala Magrurkar.
Introduction / Background
Botox injection is an effective non-surgical intervention for spastic cerebral palsy ( CP ) to decrease muscle hypertonia and bring about functional gains. Up till now motor gains have been the focused outcome of this intervention. We incidentally observed non-motor and distant gains during post botox developmental therapy programs for children injected with botox primarily for motor gains. We define distant effects as those motor gains which are not directly due to the decrease hypertonous of the targeted muscles. Distant effects have earlier been noted in the children undergoing SPR (Dr. Peacock & Dr. Purohit) & inhibitory casting ( Dr. Vikram Marwah & Dr. Shashikala ) but no such gains have been documented with botulinum administration so far. Non-motor gains are improvements in other developmental domains.
Design
Prospective and ongoing cross – sectional post intervention study.
Sample
Randomized convenient sample of 49 children with CP in the age group of 3-25 without controls.
Statistical Analysis
Percentage calculation.
Setting
Tertiary referral developmental services centre with transdiciplinary service model.
Participants And Selection Criteria
49 children with CP in the age group 3-25 years at GMFCS level I- IV were selected. The eligibility of the child and the family were evaluated on a developmental context with health related quality of life (HqOL) improvement. All the children were on Indian eclectic model of delopmental therapy for a minimum period of 6 months and maximum 14 years. GMFCS levels are indicated in
Table I:
| No. of children | GMFCS level | No. of injections |
|---|---|---|
| Total : 49 | Total : 78 | |
| 13 | I | 18 |
| 06 | II | 06 |
| 16 | III | 28 |
| 14 | IV | 26 |
Approach
currently available best clinical practice criteria for botulimun toxin injections. Method being multilevel single muscle or multilevel multi muscle injection .
Method
49 children with CP in the age group 3-25 years were evaluated clinically by administering GMFM -88 , clinical observation gait scale (COGS) , Physician Rating Scale for upper extremity function & dyanamic EMG for selection of muscles. Botox was administered under analgosedation with a broad dose range of 5- 20 units / kg. body weight and single total dose not exceeding 300 units. Children also received intensive developmental therapy after the second post injection day for a period of 1-1 ½ hours 6 days a week for the duration of 6 weeks and gains in all the developmental domains were recorded and followed up.
Results
Results are tabulated as follows –
Table : II
| Age Group | No. of children | No. of injections | No of children showing non-motor / distant gains |
|---|---|---|---|
| Total | 49 | 78 | 41 |
| 2-5 | 28 | 36 | 22 |
| 5-10 | 14 | 31 | 13 |
| 10-15 | 05 | 08 | 04 |
| 15-25 | 02 | 03 | 02 |
Table : III
| Type of gains | Percentage |
|---|---|
| Pain in back and thighs | 2.08 |
| Distant | 56.03 |
| -Fine motor (without upper limb injection) | 44 |
| – Non-motor | |
| Behavior | 42 |
| Speech | 39.5 |
| School Performance | 08.3 |
| Perception | 4.2 |
| Constipation | 2.08 |
| Feeding | 2.08 |
| Startle response | 2.08 |
| Enuresis | 2.08 |
Our results suggest distant gains in 56.3 %, fine motor improvement without injections to upper limb muscles in 44% and improvement in behavior and emotional status ( co-operative and compliant to therapy schedules , voluntarily participative, happy & decreased crying ) in 42%.
However , these effects are not dose dependent and we could not predict them. In some, the benefits have been cumulative with each injection episode and have been maintained for over a period of 4 years.
Discussion
Neurophysiologically, this may be due to the coupling of developmental events because of parallel information processing and cross talk between the processing pathways. It suggests that motor learning is a global phenomenon. The distant effects may be because of the free flow of information across the nervous system. The persistence of an infantile spinal cord with excessive intersegmental connections have been a well documented feature in CP .
Similarly fine motor improvement, when lower limb muscles alone are injected may be due to –
- Reflex inhibition
- Stable background posture
- Decreased overflow spasticity
- Neuro-mechano-temporal advantage because of improved motor recruitment
- Improved freedom of movement
- Improved motor strategies and motor learning
Conclusion
Spasticity has a wider developmental implications then just affecting the motor functions. We hereby present a hypothesis, that in children developmental domains and learning are extremely interconnected and coupled( CHIN-INDIA phenomenon). An improvement in one area can have an offshoot benefit in other areas which is important for achieving global development of children, with implications for organizing developmental programmes by therapist.
Recommendations
Therapy programmes should have more global developmental frame work using primary gross motor improvement due to decreased spasticity.