
Disable Preloader
FAQs
- History Of IACP
- Constitution Of IACP
- Executive Members
- Membership
- Annual Conference
- Fellowship Opportunities
- IJCP Journal
- Research-Priorities
- CP Day Celebration Gallery
- Government Facilities
- Join Now
- Tutorials
- Family Forum
- Book Review
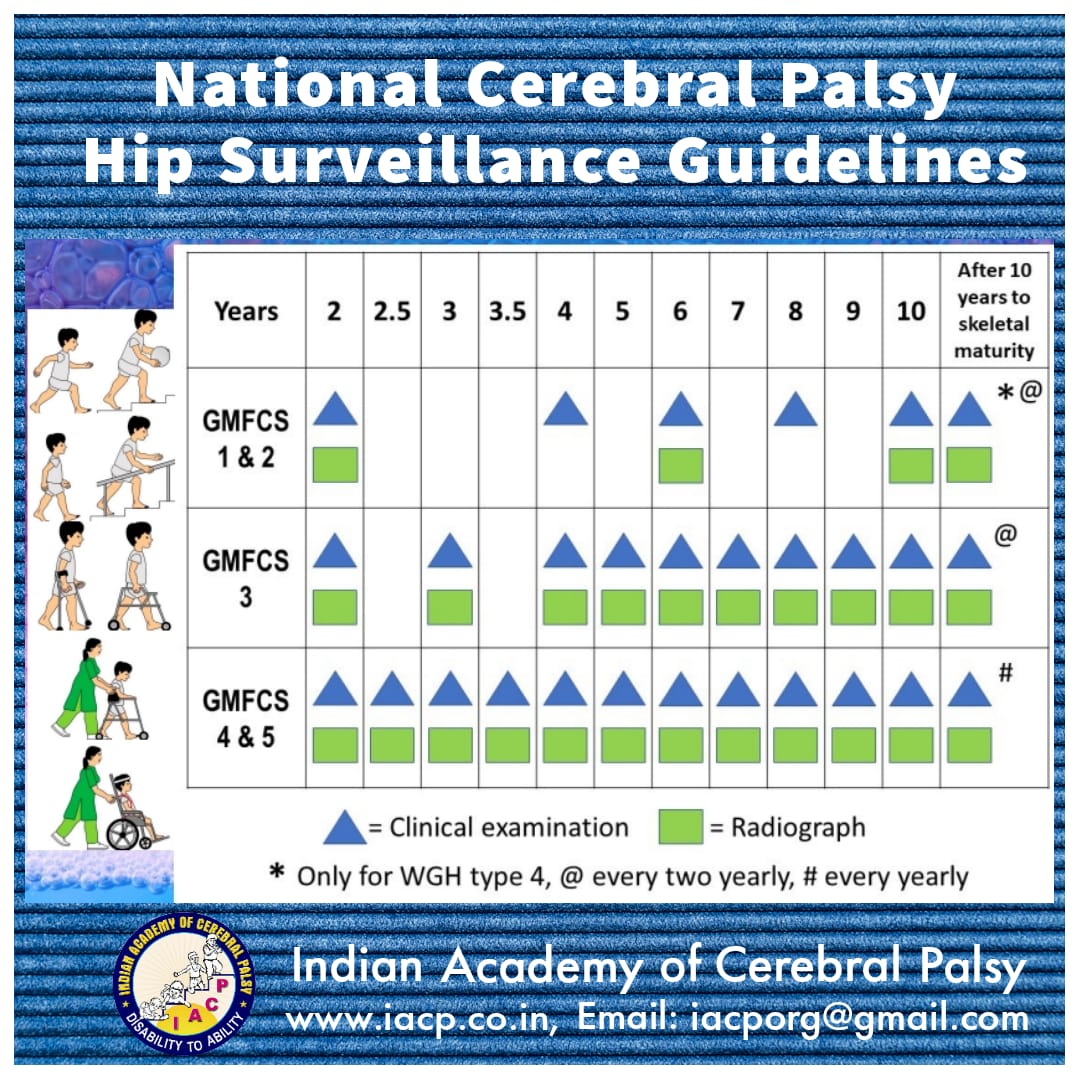
- National Cerebral Palsy Hip Surveillance Guidelines
- CP hip surveillance guidelines
- CP hip surveillance review
{kind=link}
Common Questions Of Families & Answers
Q-01 What is cerebral palsy?
Ans – Without trying to go into medical terminology in plain terms it is any injury to the developing brain of the child from conception to age 5 years ,thus cerebral palsy can occur at anytime when the child is in the mothers womb ,at the time of delivery ,just after the delivery or till the age of 5 years
Q-02 What are the causes of cerebral palsy?
Ans – The causes can be multifold from
- Prematurity
- Low birth weight ( < 2.5kg )
- Maternal epilepsys
- Hyperthyroidism
- Infection in mother
- Bleeding in 6-9 month of pregnancy
- BP in pregnancy
- Hyperthyroidism
- Drugs
- Traumas
- Multiple pregnancy
- Prolonged labor (childbirth)
- Difficult childbirth
- Bleeding during pregnancy
- Early rupture of sac
- Decreased oxygen to child during birth
- Delayed cry,child turning blue
- Prolonged jaundice
- Mother`s water goes into child’s air pipe and chokes him
Q-03 Can we find out what caused this condition in our child?
Ans – Unfortunately for all of us this is at the moment almost an impossible task, even with the best available technology and gadgetry we can just find out the cause in maximum approximately 30% out of a hundred percent children suffering from the disease ,but even this value of 30% is in research settings, in clinical settings in the west this is some where around the tune of 10-15% in south east asian countries this is 5-10% ,for a lot of parents on this journey a lot of precious resources are down the drain with no tangible results ,the best things to do are to find out if the child has any treatable cause of cerebral palsy for example congenital hypothyroidism and or a genetic cause which can lead to brain damage
Q-04 If I have one child with cerebral palsy then what are the chances that I will have another child with the same problem?
Ans – Thankfully for all of us most cases of cerebral palsy are not genetic in origin so in case you have one child with problem the chances of second child having the same problem is very slim though we need to check with the genetic counselor whether there is any genetic cause, thankfully for us we have a very good geneticist in the team who is from SGPGI and works in close collaboration with us.
In addition if your previous pregnancy has been troublesome then we need to be cautious if there is any cause why the mother’s body is unable to support the child in which case the chances of these problems increase, we also have the services of many gynecological surgeons who have training in management of such high risk deliveries
In addition if your previous pregnancy has been troublesome then we need to be cautious if there is any cause why the mother’s body is unable to support the child in which case the chances of these problems increase, we also have the services of many gynecological surgeons who have training in management of such high risk deliveries
Q-05 Can cerebral palsy be prevented?
Ans – The latest research on cerebral palsy prevention presented in the AACPDM meeting in 2008 focused on what we have learnt in terms of prevention in the last 6 decades.
Better care when the child is in the womb and prevention of infections including gynecological infections is important.
Most children who have cerebral palsy have had poor maternal history during the time that the child was in womb and that cerebral palsy is not usually the fault of the gynecologist or the pediatrician, they had problems not because the nursing team were not able to manage them but because in most cases the newborns had preexisting problems due to which they were finding it difficult to tide over in contrast to normal newborns.
The brain damage that has happened just before birth and/or just after birth can be reduced by inducing hypothermia-reducing the temperature of the body but it needs a lot of expertise on the behalf of the treating pediatrician/neonatologist.
The only method has the potential to prevent cerebral palsy has recently been documented ,taking MAGNESIUM TABLETS during the entire duration of pregnancy has been shown to be to reduce the number of spontaneous abortions ,bleeds during pregnancy and the risk of cerebral palsy, the only problem though is the availability.
in case you have trouble Mr sanjeev Prasad -091-9335901715 can be contacted over the phone and he will be able to help you, magnesium tablets are absolutely safe during pregnancy and magnesium is a metal just as calcium and iron.
Better care when the child is in the womb and prevention of infections including gynecological infections is important.
Most children who have cerebral palsy have had poor maternal history during the time that the child was in womb and that cerebral palsy is not usually the fault of the gynecologist or the pediatrician, they had problems not because the nursing team were not able to manage them but because in most cases the newborns had preexisting problems due to which they were finding it difficult to tide over in contrast to normal newborns.
The brain damage that has happened just before birth and/or just after birth can be reduced by inducing hypothermia-reducing the temperature of the body but it needs a lot of expertise on the behalf of the treating pediatrician/neonatologist.
The only method has the potential to prevent cerebral palsy has recently been documented ,taking MAGNESIUM TABLETS during the entire duration of pregnancy has been shown to be to reduce the number of spontaneous abortions ,bleeds during pregnancy and the risk of cerebral palsy, the only problem though is the availability.
in case you have trouble Mr sanjeev Prasad -091-9335901715 can be contacted over the phone and he will be able to help you, magnesium tablets are absolutely safe during pregnancy and magnesium is a metal just as calcium and iron.
Q-06 What are the associated problems that are present?
Ans –
- Visual problems
- Intellectual impairments
- Learning disabilities
- Hearing problem
- Problem in speech & communication
- Oro-motor
- Inability to chew food/gulp food
- Teeth problem
- Problem in breathing
- Problem in control of stool
- Emotional disturbances
- Drooling
- Problem in breathing
- Seizures
- For normal people slight loss of hearing or seeing ability does not matter much as they have normal brain to understand and to make up for these deficiencies but for a child with CP these difficulties with a brain injury make it difficult to understand the world leading to further impairment of mental potential.
- A lot of children have constipation but is overlooked it is uncomfortable to the child ,increases muscles spasticity or (tightness) Imagine yourself being constipated to understand how irritating it is for the child specially some one who cannot express himself.
- 30% to 65% children have mental retardation, children with intellectual impairment need special educators.
- 40% of children have some problem in vision. Ranging from blindness, myopia,or weak eye sight or squint(cross eyes).
- 10% of children have problem of hearing. Children born before time (premature)are at higher risk. All babies should be tested for hearing loss.
Q-07 How many children are suffering from CP in India?
Ans – According to conservative estimates 25 lakh children are suffering from CP in the country. Every day 150 more children are falling prey to it . It is to be marked that with our gross underreporting and poverty we may be looking at 2-3 times these numbers in reality situation
Q-08 My child is not tight is he/she a case of cerebral palsy?
Ans – Unfortunately cerebral palsy has always been associated with the the tight or spastic type,which is 70-80% of the total number,the other varieties constitute the rest,the types of cerebral palsy are:
- Spastic-muscles are tight
- Dyskinetic-muscles are sometimes tight, sometimes loose
- Hypotonic/ataxic-muscles are loose
- Mixed-tight in some part of body and loose in others| combination of above
Q-09 Can you grade my child ,how bad is he ? Is he mild ,moderate or severe?
Ans – The best answer to this can be made from by using a wonderful tool called as the GMFCS scale, we have that printed below Body support walker – A mobility device that supports the pelvis and trunk. The child/youth is physically positioned in the walker by another person.
Hand-held mobility device – Canes, crutches, and anterior and posterior walkers that do not support the trunk during walking.
Physical assistance – Another person manually assists the child/youth to move.
Powered mobility – The child/youth actively controls the joystick or electrical switch that enables independent mobility. The mobility base may be a wheelchair, scooter or other type of powered mobility device.
Self-propels manual wheelchair – The child/youth actively uses arms and hands or feet to propel the wheels and move.
Transported – A person manually pushes a mobility device (e.g., wheelchair, stroller, or pram) to move the child/youth from one place to another.
Walks – Unless otherwise specified indicates no physical assistance from another person or any use of a hand-held mobility device. An orthosis (i.e., brace or splint) may be worn.
Wheeled mobility – Refers to any type of device with wheels that enables movement (e.g., stroller, manual wheelchair, or powered wheelchair).
LEVEL I – Walks without Limitations
LEVEL II – Walks with Limitations
LEVEL III – Walks Using a Hand-Held Mobility Device
LEVEL IV – Self-Mobility with Limitations; May Use Powered Mobility
LEVEL V – Transported in a Manual Wheelchair
Distinctions Between Levels I and II – Compared with children and youth in Level I, children and youth in Level II have limitations walking long distances and balancing; may need a hand-held mobility device when first learning to walk; may use wheeled mobility when traveling long distances outdoors and in the community; require the use of a railing to walk up and down stairs; and are not as capable of running and jumping.
Distinctions Between Levels II and III – Children and youth in Level II are capable of walking without a hand-held mobility device after age 4 (although they may choose to use one at times). Children and youth in Level III need a hand-held mobility device to walk indoors and use wheeled mobility outdoors and in the community.
Distinctions Between Levels III and IV – Children and youth in Level III sit on their own or require at most limited external support to sit, are more independent in standing transfers, and walk with a hand-held mobility device.
Children and youth in Level IV function in sitting (usually supported) but self-mobility is limited. Children and youth in Level IV are more likely to be transported in a manual wheelchair or use powered mobility.
Distinctions Between Levels IV and V – Children and youth in Level V have severe limitations in head and trunk control and require extensive assisted technology and physical assistance. Self-mobility is achieved only if the child/youth can learn how to operate a powered wheelchair.
Gross Motor Function Classification System – Expanded and Revised (GMFCS – E & R)
Between 0-2 years
LEVEL I: Infants move in and out of sitting and floor sit with both hands free to manipulate objects. Infants crawl on hands and knees, pull to stand and take steps holding on to furniture. Infants walk between 18 months and 2 years of age without the need for any assistive mobility device.
LEVEL II: Infants maintain floor sitting but may need to use their hands for support to maintain balance. Infants creep on their stomach or crawl on hands and knees. Infants may pull to stand and take steps holding on to furniture.
LEVEL III: Infants maintain floor sitting when the low back is supported. Infants roll and creep forward on their stomachs.
LEVEL IV: Infants have head control but trunk support is required for floor sitting. Infants can roll to supine and may roll to prone.
LEVEL V: Physical impairments limit voluntary control of movement. Infants are unable to maintain antigravity head and trunk postures in prone and sitting. Infants require adult assistance to roll.
between 2-4 years
LEVEL I: Children floor sit with both hands free to manipulate objects. Movements in and out of floor sitting and standing are performed without adult assistance. Children walk as the preferred method of mobility without the need for any assistive mobility device.
LEVEL II: Children floor sit but may have difficulty with balance when both hands are free to manipulate objects. Movements in and out of sitting are performed without adult assistance. Children pull to stand on a stable surface. Children crawl on hands and knees with a reciprocal pattern, cruise holding onto furniture and walk using an assistive mobility device as preferred methods of mobility.
LEVEL III: Children maintain floor sitting often by “W-sitting” (sitting between flexed and internally rotated hips and knees) and may require adult assistance to assume sitting. Children creep on their stomach or crawl on hands and knees (often without reciprocal leg movements) as their primary methods of self-mobility. Children may pull to stand on a stable surface and cruise short distances. Children may walk short distances indoors using a hand-held mobility device (walker) and adult assistance for steering and turning.
LEVEL IV: Children floor sit when placed, but are unable to maintain alignment and balance without use of their hands for support. Children frequently require adaptive equipment for sitting and standing. Self-mobility for short distances (within a room) is achieved through rolling, creeping on stomach, or crawling on hands and knees without reciprocal leg movement.
LEVEL V: Physical impairments restrict voluntary control of movement and the ability to maintain antigravity head and trunk postures. All areas of motor function are limited. Functional limitations in sitting and standing are not fully compensated for through the use of adaptive equipment and assistive technology. At Level V, children have no means of independent movement and are transported. Some children achieve self-mobility using a powered wheelchair with extensive adaptations.
4-6 years
LEVEL I: Children get into and out of, and sit in, a chair without the need for hand support. Children move from the floor and from chair sitting to standing without the need for objects for support. Children walk indoors and outdoors, and climb stairs. Emerging ability to run and jump.
LEVEL II: Children sit in a chair with both hands free to manipulate objects. Children move from the floor to standing and from chair sitting to standing but often require a stable surface to push or pull up on with their arms. Children walk without the need for a handheld mobility device indoors and for short distances on level surfaces outdoors. Children climb stairs holding onto a railing but are unable to run or jump.
LEVEL III: Children sit on a regular chair but may require pelvic or trunk support to maximize hand function. Children move in and out of chair sitting using a stable surface to push on or pull up with their arms. Children walk with a hand-held mobility device on level surfaces and climb stairs with assistance from an adult. Children frequently are transported when traveling for long distances or outdoors on uneven terrain.
LEVEL IV: Children sit on a chair but need adaptive seating for trunk control and to maximize hand function. Children move in and out of chair sitting with assistance from an adult or a stable surface to push or pull up on with their arms. Children may at best walk short distances with a walker and adult supervision but have difficulty turning and maintaining balance on uneven surfaces. Children are transported in the community. Children may achieve self-mobility using a powered wheelchair.
LEVEL V: Physical impairments restrict voluntary control of movement and the ability to maintain antigravity head and trunk postures. All areas of motor function are limited. Functional limitations in sitting and standing are not fully compensated for through the use of adaptive equipment and assistive technology. At Level V, children have no means of independent movement and are transported. Some children achieve self-mobility using a powered wheelchair with extensive adaptations
6-12 years
Level I: Children walk at home, school, outdoors, and in the community. Children are able to walk up and down curbs without physical assistance and stairs without the use of a railing. Children perform gross motor skills such as running and jumping but speed, balance, and coordination are limited. Children may participate in physical activities and sports depending on personal choices and environmental factors.
Level II: Children walk in most settings. Children may experience difficulty walking long distances and balancing on uneven terrain, inclines, in crowded areas, confined spaces or when carrying objects. Children walk up and down stairs holding onto a railing or with physical assistance if there is no railing. Outdoors and in the community, children may walk with physical assistance, a hand-held mobility device, or use wheeled mobility when traveling long distances. Children have at best only minimal ability to perform gross motor skills such as running and jumping. Limitations in performance of gross motor skills may necessitate adaptations to enable participation in physical activities and sports.
Level III: Children walk using a hand-held mobility device in most indoor settings. When seated, children may require a seat belt for pelvic alignment and balance. Sit-to-stand and floor-to-stand transfers require physical assistance of a person or support surface. When traveling long distances, children use some form of wheeled mobility. Children may walk up and down stairs holding onto a railing with supervision or physical assistance. Limitations in walking may necessitate adaptations to enable participation in physical activities and sports including self-propelling a manual wheelchair or powered mobility.
Level IV: Children use methods of mobility that require physical assistance or powered mobility in most settings. Children require adaptive seating for trunk and pelvic control and physical assistance for most transfers. At home, children use floor mobility (roll, creep, or crawl), walk short distances with physical assistance, or use powered mobility. When positioned, children may use a body support walker at home or school. At school, outdoors, and in the community, children are transported in a manual wheelchair or use powered mobility. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports, including physical assistance and/or powered mobility. Level V: Children are transported in a manual wheelchair in all settings. Children are limited in their ability to maintain antigravity head and trunk postures and control arm and leg movements. Assistive technology is used to improve head alignment, seating, standing, and and/or mobility but limitations are not fully compensated by equipment. Transfers require complete physical assistance of an adult. At home, children may move short distances on the floor or may be carried by an adult. Children may achieve selfmobility using powered mobility with extensive adaptations for seating and control access. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports including physical assistance and using powered mobility.
12-18 years
Level I: Youth walk at home, school, outdoors, and in the community. Youth are able to walk up and down curbs without physical assistance and stairs without the use of a railing. Youth perform gross motor skills such as running and jumping but speed, balance, and coordination are limited. Youth may participate in physical activities and sports depending on personal choices and environmental factors.
Level II: Youth walk in most settings. Environmental factors (such as uneven terrain, inclines, long distances, time demands, weather, and peer acceptability) and personal preference influence mobility choices. At school or work, youth may walk using a handheld mobility device for safety. Outdoors and in the community, youth may use wheeled mobility when traveling long distances. Youth walk up and down stairs holding a railing or with physical assistance if there is no railing. Limitations in performance of gross motor skills may necessitate adaptations to enable participation in physical activities and sports.
Level III: Youth are capable of walking using a hand-held mobility device. Compared to individuals in other levels, youth in Level III demonstrate more variability in methods of mobility depending on physical ability and environmental and personal factors. When seated, youth may require a seat belt for pelvic alignment and balance. Sit-to-stand and floor-to-stand transfers require physical assistance from a person or support surface. At school, youth may self-propel a manual wheelchair or use powered mobility. Outdoors and in the community, youth are transported in a wheelchair or use powered mobility. Youth may walk up and down stairs holding onto a railing with supervision or physical assistance. Limitations in walking may necessitate adaptations to enable participation in physical activities and sports including self-propelling a manual wheelchair or powered mobility.
Level IV: Youth use wheeled mobility in most settings. Youth require adaptive seating for pelvic and trunk control. Physical assistance from 1 or 2 persons is required for transfers. Youth may support weight with their legs to assist with standing transfers. Indoors, youth may walk short distances with physical assistance, use wheeled mobility, or, when positioned, use a body support walker. Youth are physically capable of operating a powered wheelchair. When a powered wheelchair is not feasible or available, youth are transported in a manual wheelchair. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports, including physical assistance and/or powered mobility.
Level V: Youth are transported in a manual wheelchair in all settings. Youth are limited in their ability to maintain antigravity head and trunk postures and control arm and leg movements. Assistive technology is used to improve head alignment, seating, standing, and mobility but limitations are not fully compensated by equipment. Physical assistance from 1 or 2 persons or a mechanical lift is required for transfers. Youth may achieve self-mobility using powered mobility with extensive adaptations for seating and control access. Limitations in mobility necessitate adaptations to enable participation
Usually we have seen that with therapy /treatment continuously we can upgrade the child by at least one gmfcs level,this depends on a lot of factors like
This is just one way to know what level your child is on clinically and this is so simple that even you can do this for yourself, we need to do this regularly just to know how much progress we have made over the last few months-
keep assessing regularly in conjunction with the team the process of treatment in cerebral palsy is prolonged and usually the children who get better are the ones who’s parents show consistency and purpose over years it is easy to loose heart but believe us in doing that you inadvertently damage the cause of the one thing that you love best-your children!!!
Hand-held mobility device – Canes, crutches, and anterior and posterior walkers that do not support the trunk during walking.
Physical assistance – Another person manually assists the child/youth to move.
Powered mobility – The child/youth actively controls the joystick or electrical switch that enables independent mobility. The mobility base may be a wheelchair, scooter or other type of powered mobility device.
Self-propels manual wheelchair – The child/youth actively uses arms and hands or feet to propel the wheels and move.
Transported – A person manually pushes a mobility device (e.g., wheelchair, stroller, or pram) to move the child/youth from one place to another.
Walks – Unless otherwise specified indicates no physical assistance from another person or any use of a hand-held mobility device. An orthosis (i.e., brace or splint) may be worn.
Wheeled mobility – Refers to any type of device with wheels that enables movement (e.g., stroller, manual wheelchair, or powered wheelchair).
LEVEL I – Walks without Limitations
LEVEL II – Walks with Limitations
LEVEL III – Walks Using a Hand-Held Mobility Device
LEVEL IV – Self-Mobility with Limitations; May Use Powered Mobility
LEVEL V – Transported in a Manual Wheelchair
Distinctions Between Levels I and II – Compared with children and youth in Level I, children and youth in Level II have limitations walking long distances and balancing; may need a hand-held mobility device when first learning to walk; may use wheeled mobility when traveling long distances outdoors and in the community; require the use of a railing to walk up and down stairs; and are not as capable of running and jumping.
Distinctions Between Levels II and III – Children and youth in Level II are capable of walking without a hand-held mobility device after age 4 (although they may choose to use one at times). Children and youth in Level III need a hand-held mobility device to walk indoors and use wheeled mobility outdoors and in the community.
Distinctions Between Levels III and IV – Children and youth in Level III sit on their own or require at most limited external support to sit, are more independent in standing transfers, and walk with a hand-held mobility device.
Children and youth in Level IV function in sitting (usually supported) but self-mobility is limited. Children and youth in Level IV are more likely to be transported in a manual wheelchair or use powered mobility.
Distinctions Between Levels IV and V – Children and youth in Level V have severe limitations in head and trunk control and require extensive assisted technology and physical assistance. Self-mobility is achieved only if the child/youth can learn how to operate a powered wheelchair.
Gross Motor Function Classification System – Expanded and Revised (GMFCS – E & R)
Between 0-2 years
LEVEL I: Infants move in and out of sitting and floor sit with both hands free to manipulate objects. Infants crawl on hands and knees, pull to stand and take steps holding on to furniture. Infants walk between 18 months and 2 years of age without the need for any assistive mobility device.
LEVEL II: Infants maintain floor sitting but may need to use their hands for support to maintain balance. Infants creep on their stomach or crawl on hands and knees. Infants may pull to stand and take steps holding on to furniture.
LEVEL III: Infants maintain floor sitting when the low back is supported. Infants roll and creep forward on their stomachs.
LEVEL IV: Infants have head control but trunk support is required for floor sitting. Infants can roll to supine and may roll to prone.
LEVEL V: Physical impairments limit voluntary control of movement. Infants are unable to maintain antigravity head and trunk postures in prone and sitting. Infants require adult assistance to roll.
between 2-4 years
LEVEL I: Children floor sit with both hands free to manipulate objects. Movements in and out of floor sitting and standing are performed without adult assistance. Children walk as the preferred method of mobility without the need for any assistive mobility device.
LEVEL II: Children floor sit but may have difficulty with balance when both hands are free to manipulate objects. Movements in and out of sitting are performed without adult assistance. Children pull to stand on a stable surface. Children crawl on hands and knees with a reciprocal pattern, cruise holding onto furniture and walk using an assistive mobility device as preferred methods of mobility.
LEVEL III: Children maintain floor sitting often by “W-sitting” (sitting between flexed and internally rotated hips and knees) and may require adult assistance to assume sitting. Children creep on their stomach or crawl on hands and knees (often without reciprocal leg movements) as their primary methods of self-mobility. Children may pull to stand on a stable surface and cruise short distances. Children may walk short distances indoors using a hand-held mobility device (walker) and adult assistance for steering and turning.
LEVEL IV: Children floor sit when placed, but are unable to maintain alignment and balance without use of their hands for support. Children frequently require adaptive equipment for sitting and standing. Self-mobility for short distances (within a room) is achieved through rolling, creeping on stomach, or crawling on hands and knees without reciprocal leg movement.
LEVEL V: Physical impairments restrict voluntary control of movement and the ability to maintain antigravity head and trunk postures. All areas of motor function are limited. Functional limitations in sitting and standing are not fully compensated for through the use of adaptive equipment and assistive technology. At Level V, children have no means of independent movement and are transported. Some children achieve self-mobility using a powered wheelchair with extensive adaptations.
4-6 years
LEVEL I: Children get into and out of, and sit in, a chair without the need for hand support. Children move from the floor and from chair sitting to standing without the need for objects for support. Children walk indoors and outdoors, and climb stairs. Emerging ability to run and jump.
LEVEL II: Children sit in a chair with both hands free to manipulate objects. Children move from the floor to standing and from chair sitting to standing but often require a stable surface to push or pull up on with their arms. Children walk without the need for a handheld mobility device indoors and for short distances on level surfaces outdoors. Children climb stairs holding onto a railing but are unable to run or jump.
LEVEL III: Children sit on a regular chair but may require pelvic or trunk support to maximize hand function. Children move in and out of chair sitting using a stable surface to push on or pull up with their arms. Children walk with a hand-held mobility device on level surfaces and climb stairs with assistance from an adult. Children frequently are transported when traveling for long distances or outdoors on uneven terrain.
LEVEL IV: Children sit on a chair but need adaptive seating for trunk control and to maximize hand function. Children move in and out of chair sitting with assistance from an adult or a stable surface to push or pull up on with their arms. Children may at best walk short distances with a walker and adult supervision but have difficulty turning and maintaining balance on uneven surfaces. Children are transported in the community. Children may achieve self-mobility using a powered wheelchair.
LEVEL V: Physical impairments restrict voluntary control of movement and the ability to maintain antigravity head and trunk postures. All areas of motor function are limited. Functional limitations in sitting and standing are not fully compensated for through the use of adaptive equipment and assistive technology. At Level V, children have no means of independent movement and are transported. Some children achieve self-mobility using a powered wheelchair with extensive adaptations
6-12 years
Level I: Children walk at home, school, outdoors, and in the community. Children are able to walk up and down curbs without physical assistance and stairs without the use of a railing. Children perform gross motor skills such as running and jumping but speed, balance, and coordination are limited. Children may participate in physical activities and sports depending on personal choices and environmental factors.
Level II: Children walk in most settings. Children may experience difficulty walking long distances and balancing on uneven terrain, inclines, in crowded areas, confined spaces or when carrying objects. Children walk up and down stairs holding onto a railing or with physical assistance if there is no railing. Outdoors and in the community, children may walk with physical assistance, a hand-held mobility device, or use wheeled mobility when traveling long distances. Children have at best only minimal ability to perform gross motor skills such as running and jumping. Limitations in performance of gross motor skills may necessitate adaptations to enable participation in physical activities and sports.
Level III: Children walk using a hand-held mobility device in most indoor settings. When seated, children may require a seat belt for pelvic alignment and balance. Sit-to-stand and floor-to-stand transfers require physical assistance of a person or support surface. When traveling long distances, children use some form of wheeled mobility. Children may walk up and down stairs holding onto a railing with supervision or physical assistance. Limitations in walking may necessitate adaptations to enable participation in physical activities and sports including self-propelling a manual wheelchair or powered mobility.
Level IV: Children use methods of mobility that require physical assistance or powered mobility in most settings. Children require adaptive seating for trunk and pelvic control and physical assistance for most transfers. At home, children use floor mobility (roll, creep, or crawl), walk short distances with physical assistance, or use powered mobility. When positioned, children may use a body support walker at home or school. At school, outdoors, and in the community, children are transported in a manual wheelchair or use powered mobility. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports, including physical assistance and/or powered mobility. Level V: Children are transported in a manual wheelchair in all settings. Children are limited in their ability to maintain antigravity head and trunk postures and control arm and leg movements. Assistive technology is used to improve head alignment, seating, standing, and and/or mobility but limitations are not fully compensated by equipment. Transfers require complete physical assistance of an adult. At home, children may move short distances on the floor or may be carried by an adult. Children may achieve selfmobility using powered mobility with extensive adaptations for seating and control access. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports including physical assistance and using powered mobility.
12-18 years
Level I: Youth walk at home, school, outdoors, and in the community. Youth are able to walk up and down curbs without physical assistance and stairs without the use of a railing. Youth perform gross motor skills such as running and jumping but speed, balance, and coordination are limited. Youth may participate in physical activities and sports depending on personal choices and environmental factors.
Level II: Youth walk in most settings. Environmental factors (such as uneven terrain, inclines, long distances, time demands, weather, and peer acceptability) and personal preference influence mobility choices. At school or work, youth may walk using a handheld mobility device for safety. Outdoors and in the community, youth may use wheeled mobility when traveling long distances. Youth walk up and down stairs holding a railing or with physical assistance if there is no railing. Limitations in performance of gross motor skills may necessitate adaptations to enable participation in physical activities and sports.
Level III: Youth are capable of walking using a hand-held mobility device. Compared to individuals in other levels, youth in Level III demonstrate more variability in methods of mobility depending on physical ability and environmental and personal factors. When seated, youth may require a seat belt for pelvic alignment and balance. Sit-to-stand and floor-to-stand transfers require physical assistance from a person or support surface. At school, youth may self-propel a manual wheelchair or use powered mobility. Outdoors and in the community, youth are transported in a wheelchair or use powered mobility. Youth may walk up and down stairs holding onto a railing with supervision or physical assistance. Limitations in walking may necessitate adaptations to enable participation in physical activities and sports including self-propelling a manual wheelchair or powered mobility.
Level IV: Youth use wheeled mobility in most settings. Youth require adaptive seating for pelvic and trunk control. Physical assistance from 1 or 2 persons is required for transfers. Youth may support weight with their legs to assist with standing transfers. Indoors, youth may walk short distances with physical assistance, use wheeled mobility, or, when positioned, use a body support walker. Youth are physically capable of operating a powered wheelchair. When a powered wheelchair is not feasible or available, youth are transported in a manual wheelchair. Limitations in mobility necessitate adaptations to enable participation in physical activities and sports, including physical assistance and/or powered mobility.
Level V: Youth are transported in a manual wheelchair in all settings. Youth are limited in their ability to maintain antigravity head and trunk postures and control arm and leg movements. Assistive technology is used to improve head alignment, seating, standing, and mobility but limitations are not fully compensated by equipment. Physical assistance from 1 or 2 persons or a mechanical lift is required for transfers. Youth may achieve self-mobility using powered mobility with extensive adaptations for seating and control access. Limitations in mobility necessitate adaptations to enable participation
Usually we have seen that with therapy /treatment continuously we can upgrade the child by at least one gmfcs level,this depends on a lot of factors like
- Timing of achievement of landmarks.
- Severity of development landmarks.
- Degree of intellectual involvement.
- Sensory perception. of the child to his/her surroundings
- Motivation in child to move / explore the world.
- Family support of the parents and the grandparents
- Environment factors
- Presence/absence of fits –children who have fits do not progress as fast as children who don’t Repeated chest infections- children who have repeated cough cold do not progress as fast as children who don’t
- Body awareness.
- Ability to plan| execute function.
- Behavior / cooperation of the child .
- Medical problems
This is just one way to know what level your child is on clinically and this is so simple that even you can do this for yourself, we need to do this regularly just to know how much progress we have made over the last few months-
keep assessing regularly in conjunction with the team the process of treatment in cerebral palsy is prolonged and usually the children who get better are the ones who’s parents show consistency and purpose over years it is easy to loose heart but believe us in doing that you inadvertently damage the cause of the one thing that you love best-your children!!!
Q-10 what is the future of my child will he be able to walk and when?
Ans – This is the most common question that we as professionals have to answer and also the most tricky one, answering this is like looking into the wishing glass and telling the future and answers to this is the source of the biggest confusion and disenchantment with professionals ,some doctors will tell you looking at the child at birth that nothing can be done and this child will never be able to do anything in life causing immense depression to parents who are young and have just started life together on the other end of the spectrum are parents who have been told that everything is okay and the child will be absolutely normal be a little slow in achieving their milestones, there are others who have lost a lot of time, effort and a lot of resources over claims by professionals that they will be able to make the child sit/stand /walk in 3 months /6 months most of these claims are usually false and cause depression/resentment in parents
The usual answer to this question that I feel is being truthful and telling that –WE DON’T KNOW!!!
The problem is that this is very difficult for professionals to accept this fact but the truth is as parents/individuals you don’t know what is your future going to be 5 years from now, where will you be 5 years down the lane ,what will be your income 5 years from now, what will be the physical status of your health 5 years from now
Just as this is so difficult to tell and predict such is the difficulty that professionals have in answering this question and any definite prediction is going to fall into either of the two categories a) over positive b) over negative
The best method is assessing where the child is today and then make 6 monthly goals or yearly goals after sitting with the team of professionals wherein each professional knows what is expected out from him/her this is just like the school does when we send our kids to them ,gives them daily lessons and assesses them weekly/monthly/quarterly/half yearly and yearly and just as we don’t know whether some child who has been sent to school will turn out to be an great leader or a plumber we don’t know what will your child become when we assess them the first time we can make valid assessments only when we see them and assess them regularly
The answer then is
Sit with the team of professionals
Find out what level your child is –TODAY
Find out his strengths and also his weakness ie – IDENTIFY THE PROBLEM AREAS
Make 6 monthly and half yearly –REALISTIC GOALS
Assess with the team-AT REGULAR INTERVALS
There is a scale/tool called as the GMFM which can help us to assess them at 6 monthly intervals and tell us where have we gone, in addition we also have developed in conjunction with SGPGI ,LUCKNOW a new method of assessment called as Diffusion Tensor Imaging(DTI) , it tells us at regular intervals what are we looking at today and at 6 months reassessing WHERE WE HAVE REACHED
So we have 3 methods of assessment
Repeated clinical assessment
Repeated video assessment
Repeated diffusion tensor imaging assessment
Having multiple tools of assessment helps us validate all the tools against each other making better assessments.
All that we have said earlier is true for children below the age of 6 years ,once they have crossed this age making a statement will become easier ,we can say with a reasonable degree of confidence where this child is going to be 5 years from now this is because the curves in the GMFM scales flatten out, the brains plasticity or growth potential is smaller and the children start showing their true potentials
The usual answer to this question that I feel is being truthful and telling that –WE DON’T KNOW!!!
The problem is that this is very difficult for professionals to accept this fact but the truth is as parents/individuals you don’t know what is your future going to be 5 years from now, where will you be 5 years down the lane ,what will be your income 5 years from now, what will be the physical status of your health 5 years from now
Just as this is so difficult to tell and predict such is the difficulty that professionals have in answering this question and any definite prediction is going to fall into either of the two categories a) over positive b) over negative
The best method is assessing where the child is today and then make 6 monthly goals or yearly goals after sitting with the team of professionals wherein each professional knows what is expected out from him/her this is just like the school does when we send our kids to them ,gives them daily lessons and assesses them weekly/monthly/quarterly/half yearly and yearly and just as we don’t know whether some child who has been sent to school will turn out to be an great leader or a plumber we don’t know what will your child become when we assess them the first time we can make valid assessments only when we see them and assess them regularly
The answer then is
Sit with the team of professionals
Find out what level your child is –TODAY
Find out his strengths and also his weakness ie – IDENTIFY THE PROBLEM AREAS
Make 6 monthly and half yearly –REALISTIC GOALS
Assess with the team-AT REGULAR INTERVALS
There is a scale/tool called as the GMFM which can help us to assess them at 6 monthly intervals and tell us where have we gone, in addition we also have developed in conjunction with SGPGI ,LUCKNOW a new method of assessment called as Diffusion Tensor Imaging(DTI) , it tells us at regular intervals what are we looking at today and at 6 months reassessing WHERE WE HAVE REACHED
So we have 3 methods of assessment
Repeated clinical assessment
Repeated video assessment
Repeated diffusion tensor imaging assessment
Having multiple tools of assessment helps us validate all the tools against each other making better assessments.
All that we have said earlier is true for children below the age of 6 years ,once they have crossed this age making a statement will become easier ,we can say with a reasonable degree of confidence where this child is going to be 5 years from now this is because the curves in the GMFM scales flatten out, the brains plasticity or growth potential is smaller and the children start showing their true potentials
Q-11 Can we change the brain /can we repair the brain damage?
Ans – Thankfully for us the answer is YES!!!
The brain in children starts to repair itself immediately after an injury ,this is increased by the brains capacity to mould itself from learned experiences which is called as plasticity, the brain has maximum plasticity from just after birth till about the age of 5-6 years which is why cerebral palsy does occur till that age and which is exactly why it is best treated in that age, till the watershed age of 6 all treatments have a more lasting effect on the brain and then the plasticity drops ,though it doesn’t become zero
We have for the first time in the world demonstrated the effect of treatment with botulin toxin(DYSPORT @ IPSEN UK) on the brain plasticity ,we injected DYSPORT to the hyperactive muscles and then followed the children’s brain with serial Diffusion tensor imaging( DTI) at SGPGI, Lucknow to the surprise of the lead investigator Dr R.K.GUPTA the specialist at SGPGI ,MRI DEPARTMENT we found that the brains of children who were given DYSPORT were becoming better, this research was published in pediatric neurology
Treatment-Induced Plasticity in Cerebral Palsy: A Diffusion Tensor Imaging Study Pediatric Neurology – Volume 39, Issue 5 (November 2008) Richa Trivedi, PhD Rakesh K. Gupta – MD, Vipul Shah – MS, Mukesh Tripathi – MD, RamK.S. Rathore – PhD, Manoj Kumar – MSc, Chandra M. Pandey – PhD, Ponnada A. Narayana – PhD
So if you have a child below 5 the answer is pick up your reserves and start working hard today because the CHANCE IS TODAY!!!
The brain in children starts to repair itself immediately after an injury ,this is increased by the brains capacity to mould itself from learned experiences which is called as plasticity, the brain has maximum plasticity from just after birth till about the age of 5-6 years which is why cerebral palsy does occur till that age and which is exactly why it is best treated in that age, till the watershed age of 6 all treatments have a more lasting effect on the brain and then the plasticity drops ,though it doesn’t become zero
We have for the first time in the world demonstrated the effect of treatment with botulin toxin(DYSPORT @ IPSEN UK) on the brain plasticity ,we injected DYSPORT to the hyperactive muscles and then followed the children’s brain with serial Diffusion tensor imaging( DTI) at SGPGI, Lucknow to the surprise of the lead investigator Dr R.K.GUPTA the specialist at SGPGI ,MRI DEPARTMENT we found that the brains of children who were given DYSPORT were becoming better, this research was published in pediatric neurology
Treatment-Induced Plasticity in Cerebral Palsy: A Diffusion Tensor Imaging Study Pediatric Neurology – Volume 39, Issue 5 (November 2008) Richa Trivedi, PhD Rakesh K. Gupta – MD, Vipul Shah – MS, Mukesh Tripathi – MD, RamK.S. Rathore – PhD, Manoj Kumar – MSc, Chandra M. Pandey – PhD, Ponnada A. Narayana – PhD
So if you have a child below 5 the answer is pick up your reserves and start working hard today because the CHANCE IS TODAY!!!
Q-12 What is the role of therapy in the treatment is physiotherapy better or occupational therapy better?
Ans – The effects of both are truly complimentary ,none is better than the other while physiotherapists are good at stretching the muscles and increasing strength of the muscles by using electro stimulation ,occupational therapists are good at training the injured brain to function by doing and redoing tasks just as repeatedly writing something when in school enhances your recalling power the problem however is that both of them usually have problems accepting the other’s strength, treatment of cerebral palsy is always and will always remain MULTIDISCIPLINARY and will need everyone to pool their resources and efforts all of us whether it is parents, therapists, pediatricians ,neurologists and the pediatric orthopedic surgeon have to pool their efforts along with other ancillary team members including the educator /orthotics specialist and or the speech therapist
NO ONE CAN DO IT ALL !!!!!!!!!!! .
NO ONE CAN DO IT ALL !!!!!!!!!!! .
Q-13 What is the role of alternative therapies in cerebral palsy can I do homeopathy, ayurvedic also?
Ans – The stance that I have always taken is that we have little idea on the role of these treatment modalities; they are a world into themselves the only problem with use of these modalities is that we have no reports which have validated these treatments so we can never check the authenticity of these claims , if you believe that these treatments can help your child please go ahead and do it but do not leave time tested modalities that are proved to help children with cerebral palsy for these treatments just add on
Q-14 Will treatment of the body treat the brain?
Ans – Yes it does!
We in addition to doing treatment do a lot of therapy; this therapy will change the brain by acting on plasticity or the capacity of the brain to mould /change and repair itself after an injury
We in addition to doing treatment do a lot of therapy; this therapy will change the brain by acting on plasticity or the capacity of the brain to mould /change and repair itself after an injury
Q-15 How much therapy (physiotherapy) is ideally needed?
Ans – It has been proved by research that ideally muscle needs to be kept stretched for 6 hours to keep it in lengthened position now this is a difficult thing to do, no therapist can spend such time with your kid so in the end the onus comes onto parents and the family, as a team we have always believed that the family has to be motivated to bridge the gap in the duration The family needs to put in at least 2 hours of therapy everyday, in addition to the therapists efforts
In addition the kids have to wear splints for 6-8 hours a day to maintain the muscles in lengthened position, in case children do not wear splints the main cause is spasticity or tightness
In addition the kids have to wear splints for 6-8 hours a day to maintain the muscles in lengthened position, in case children do not wear splints the main cause is spasticity or tightness
Q-16 Why do children get spastic?
Ans – This is because in normal children the muscles and the bones maintain a ratio of equal length gain during the time of growth therefore maintaining equilibrium in children with cerebral palsy unfortunately this equilibrium is hampered and therefore the bones keep on growing while the muscles don’t, every time the child grows this discrepancy gets exaggerated ,initially this leads to tightness in muscles ,later getting converted to fixed non stretchable changes in muscles and later permanent bony changes
Q-17 I have been told that my child needs surgery of the tendo Achilles ,he is 5 should I get it done?
Ans – Absolutely not! We have just explained to you the process of generation of tightness in the muscles, so children whenever they gain height are prone to getting shorter muscles they keep on adding height in boys upto the age of 14-15 in boys and upto 10/11 in girls ,but the major growth ends by the age of 9/10 so ideally we should not do surgery before 9/10 in children with cerebral palsy as they are doomed to having greater potential of failure and or major weakness We now have better methods in our fight against spasticity than surgery The only 2 surgeries that can be done before the child is 10 are:
1) the adductor tenotomies/ lengthening for scissoring during standing/walking
2) the pronator lengthening or transfer in the arm to allow children to show their palm
1) the adductor tenotomies/ lengthening for scissoring during standing/walking
2) the pronator lengthening or transfer in the arm to allow children to show their palm
Q-18 what are the treatment modalities before the child is 10 years?
Ans – The major modalities are: Therapy (both physio and occupational)
Tone reducing special plasters
Oral anti spastic drugs like tizanidine and baclofen
Botulin toxin (DYSPORT ) injections in the muscles which are spastic
Surgery in the form of
the adductor tenotomies/ lengthening for scissoring during standing/walking
the pronator lengthening or transfer in the arm to allow children to show their palm
Rarely (less than 1%) can the child need dorsal rhizotomies, these are done on the spine and can reduce spasticity in children the side effect is that they can lead to permanent weakness in the muscles and that is why they are usually avoided
Tone reducing special plasters
Oral anti spastic drugs like tizanidine and baclofen
Botulin toxin (DYSPORT ) injections in the muscles which are spastic
Surgery in the form of
the adductor tenotomies/ lengthening for scissoring during standing/walking
the pronator lengthening or transfer in the arm to allow children to show their palm
Rarely (less than 1%) can the child need dorsal rhizotomies, these are done on the spine and can reduce spasticity in children the side effect is that they can lead to permanent weakness in the muscles and that is why they are usually avoided
Q-19 Treatment modalities after the child is 10 ?
Ans – The treatment then slowly shifts to surgery(MULTILEVEL) and therapy in conjunction to surgery as the primary modality and the other modalities then start becoming secondary
the decision to doing surgery should never be taken in the first meeting and all efforts should be made to understand the body of the child and making decisions taking all members of the team into confidence before undertaking the process
The goals of what will be achieved by surgery should be known and perfectly understood by all ,the team usually comprises of
The commander in chief – the mother of the child
The therapist
The pediatric orthopedic surgeon
The other family members including the father
The orthotist, the special educator and all those who are involved in caring for the child
the decision to doing surgery should never be taken in the first meeting and all efforts should be made to understand the body of the child and making decisions taking all members of the team into confidence before undertaking the process
The goals of what will be achieved by surgery should be known and perfectly understood by all ,the team usually comprises of
The commander in chief – the mother of the child
The therapist
The pediatric orthopedic surgeon
The other family members including the father
The orthotist, the special educator and all those who are involved in caring for the child
Q-20 How much time does it take to recover after MULTILEVEL surgery?
Ans – Normally children are in supportive cast after surgery for a period of 6 weeks after which the cast is off and the process of therapy is started rigorously,
In all surgeries children loose a little muscular power and therefore it makes sense to be doing intensive therapy even before the surgery ,typically the total period which the child needs post surgery to get good results of surgery is approximately an year so before we need to take decision on when to do surgery all members of the team should be geared to working hard for a period of at least 1 year
In all surgeries children loose a little muscular power and therefore it makes sense to be doing intensive therapy even before the surgery ,typically the total period which the child needs post surgery to get good results of surgery is approximately an year so before we need to take decision on when to do surgery all members of the team should be geared to working hard for a period of at least 1 year
Q-21 What are the goals of surgery or botulin injections?
Ans – The usual goals of surgery are
To allow the child to sit better
To allow the child to sit comfortably without pain
To allow the child to stand with/without support
To allow the child to walk with/without support
To allow the child to walk better
Allow the child to use their hands better
The final decision on what is the appropriate initial goal for your child should be made by all the team members sitting together ,make realistic goals and then work hard to attain them
To allow the child to sit better
To allow the child to sit comfortably without pain
To allow the child to stand with/without support
To allow the child to walk with/without support
To allow the child to walk better
Allow the child to use their hands better
The final decision on what is the appropriate initial goal for your child should be made by all the team members sitting together ,make realistic goals and then work hard to attain them
Q-22 How early can my child be given botulin?
Ans – A we have seen a very good safety profile for DYSPORT ,and have given it to children as young as a year in cerebral palsy, for children with other diseases like Erb`s palsy we have given the injection to children as young as 3-4 months, without any side effects
The catch always is and will remain is that botulin will work best when the child is having plasticity in the brain ie below 5 years ,the only problem though is that many children loose this opportunity because the parents are either misguided or because of the fact that they are too afraid to take this step but if you come to the clinic and meet other parents like you who`s children have been tremendously benefitted by botulin then you will realize what chance are you deriving your child from
If you send in a request then we will be happy to provide you the numbers of parents who will be able to share their experiences with you.
The catch always is and will remain is that botulin will work best when the child is having plasticity in the brain ie below 5 years ,the only problem though is that many children loose this opportunity because the parents are either misguided or because of the fact that they are too afraid to take this step but if you come to the clinic and meet other parents like you who`s children have been tremendously benefitted by botulin then you will realize what chance are you deriving your child from
If you send in a request then we will be happy to provide you the numbers of parents who will be able to share their experiences with you.
Q-23 Will botulin shot given to my child last for life?
Ans – Botulin is a drug and like all drugs will last for a period, in this case roughly for a period of 6 months, the best part is that its effect can be increased by giving plasters along with the drug
The duration of effect depends on so many factors
1. the age of the child – the younger the child the longer is the effect
2. how much therapy does the child get
3. how much splints does the child wear
4. what is the frequency of fits in the child
5. what is the frequency that the child gets cough and cold and subsequently skips therapy
6. whether the child cooperates with the post botulin exercise schedule
If all goes well and the child is young we have seen this effect stay for as long as 2 years ,but usually we are able to stretch it upto 1-1.5 years
The duration of effect depends on so many factors
1. the age of the child – the younger the child the longer is the effect
2. how much therapy does the child get
3. how much splints does the child wear
4. what is the frequency of fits in the child
5. what is the frequency that the child gets cough and cold and subsequently skips therapy
6. whether the child cooperates with the post botulin exercise schedule
If all goes well and the child is young we have seen this effect stay for as long as 2 years ,but usually we are able to stretch it upto 1-1.5 years
Q-24 What is the incidence of eye problems in such children and what should I do about this?
Ans – Only 20-25% children with cerebral palsy have perfectly normal eyes. 40% of children have refractory errors ie have need of glasses
Squint is found in over 50% children with cerebral palsy ie the axis of the eye is deviated ,considering only 2-3% of normal children have such a problem this is obviously a very high percentage Nystagmus or constantly moving eye was found in 16% ,more in dystonic or ataxic patients most children who can follow instructions will benefit with prisms and corrective excercises,if this doesn’t help then surgery is the only option
Taking into consideration the age of the patient, the strabismus /squint surgery targets different things. In preschool children, we operate aiming the recovery of the binocular vision, while in children over ten years old, the surgery is done only for cosmetic reasons.
The key to betterment usually lies in quicker diagnosis, see a good ophthalmologist as soon as your child is diagnosed with cerebral palsy
Squint is found in over 50% children with cerebral palsy ie the axis of the eye is deviated ,considering only 2-3% of normal children have such a problem this is obviously a very high percentage Nystagmus or constantly moving eye was found in 16% ,more in dystonic or ataxic patients most children who can follow instructions will benefit with prisms and corrective excercises,if this doesn’t help then surgery is the only option
Taking into consideration the age of the patient, the strabismus /squint surgery targets different things. In preschool children, we operate aiming the recovery of the binocular vision, while in children over ten years old, the surgery is done only for cosmetic reasons.
The key to betterment usually lies in quicker diagnosis, see a good ophthalmologist as soon as your child is diagnosed with cerebral palsy
Q-25 how do I get the best result of botulin?
Ans – Very often I see so called failures of botulin toxin and we have tried analyzing why that has happened the major reasons as we have found are:
Physicians have not spent time analyzing the child before injecting botulin,if your physician has not spent at least 30 -45 minutes in analyzing the problems of your child the chances that he/she will not do a good job are very high
a lot of parents have had their children given botulin shots in camps,such camp mentality usually harms because-
a) children are not evaluated well by the physician
b) the physician comes on a flying visit ,injects and leaves leaving the followup to either the therapist or to parents and never cares for reevaluating the child again
c) the dosages are not given well
d) the child is usually not fully asleep and the drug doesn’t reach the correct spot
e) the hype that is created is that this one shot will cure your child from cerebral palsy or that your child will start walking after the shot no one talks about how hard you have and or your therapist has to work
f) nobody cares about the splints
g) plasters may not be given when they are needed
SO THINK 10 TIMES BEFORE YOU ALLOW YOUR CHILD TO GET A SHOT IN CAMP SETTING
the third most common cause of so called failures is that as a parent you are not educated about the efforts that you have to make ,your child needs at least 3 hours of therapy and splints the next most common cause of so called failure is because the child may need a plaster in addition to botulin which he may not have received
the last cause of so called failure is because that you aren’t informed and you expect your child to be cured of cerebral palsy by one shot of botulin which it will not, it is a drug and has its effect the duration may be prolonged by doing it well, adding plasters, giving oral drugs, wearing splints and wearing splints
Physicians have not spent time analyzing the child before injecting botulin,if your physician has not spent at least 30 -45 minutes in analyzing the problems of your child the chances that he/she will not do a good job are very high
a lot of parents have had their children given botulin shots in camps,such camp mentality usually harms because-
a) children are not evaluated well by the physician
b) the physician comes on a flying visit ,injects and leaves leaving the followup to either the therapist or to parents and never cares for reevaluating the child again
c) the dosages are not given well
d) the child is usually not fully asleep and the drug doesn’t reach the correct spot
e) the hype that is created is that this one shot will cure your child from cerebral palsy or that your child will start walking after the shot no one talks about how hard you have and or your therapist has to work
f) nobody cares about the splints
g) plasters may not be given when they are needed
SO THINK 10 TIMES BEFORE YOU ALLOW YOUR CHILD TO GET A SHOT IN CAMP SETTING
the third most common cause of so called failures is that as a parent you are not educated about the efforts that you have to make ,your child needs at least 3 hours of therapy and splints the next most common cause of so called failure is because the child may need a plaster in addition to botulin which he may not have received
the last cause of so called failure is because that you aren’t informed and you expect your child to be cured of cerebral palsy by one shot of botulin which it will not, it is a drug and has its effect the duration may be prolonged by doing it well, adding plasters, giving oral drugs, wearing splints and wearing splints
Q-26 How much time does it take to give botulin?
Ans – We normally examine your child at least for 40-45 minutes ,examine his walking pattern by video gait analysis, examine his muscle strength and then may tell you that your child will need botulin
Some time we may call you for one /two more appointments to firm up our decision As a policy we have always believed that we need to understand your child fully well before we do your botulin ,may be ensure that you have a good therapist, check out your splints and or see the effect of oral drugs
DOING BOTULIN IS EXPENSIVE –NOT ONLY IN TERMS OF MONEY BUT ALSO IN TERMS OF THE EEFORTS THAT ALL OF US WILL NEED TO PUT
WE HAVE ALWAYS BELIEVED THAT RESOURCES WHETHER YOURS OR OURS SHOULD NOT BE WASTED AND WE WILL ENBSURE THAT WHEN WE DO BOTULIN FOR YOUR CHILD WE TAKE ALL EFFORTS TO ENSURE THAT THE KID GETS THE BEST OUT OF THE TREATMENT !!
Some time we may call you for one /two more appointments to firm up our decision As a policy we have always believed that we need to understand your child fully well before we do your botulin ,may be ensure that you have a good therapist, check out your splints and or see the effect of oral drugs
DOING BOTULIN IS EXPENSIVE –NOT ONLY IN TERMS OF MONEY BUT ALSO IN TERMS OF THE EEFORTS THAT ALL OF US WILL NEED TO PUT
WE HAVE ALWAYS BELIEVED THAT RESOURCES WHETHER YOURS OR OURS SHOULD NOT BE WASTED AND WE WILL ENBSURE THAT WHEN WE DO BOTULIN FOR YOUR CHILD WE TAKE ALL EFFORTS TO ENSURE THAT THE KID GETS THE BEST OUT OF THE TREATMENT !!
Q-27 What is the process of giving botulin?
Ans – We will normally call your child and under a little sleep give him botulin this may or may not be accompanied with plasters and after this you stay in the hospital for just 4 hours when your child gets up and then you can leave
In case your child has had a plaster with botulin then we will call him after a period of 6 weeks when we cut the plaster and then therapy starts
In case it is only botulin and no plaster then we will probably call him/her in 3 weeks to assess and then regularly
If you have any other question e mail us
In case your child has had a plaster with botulin then we will call him after a period of 6 weeks when we cut the plaster and then therapy starts
In case it is only botulin and no plaster then we will probably call him/her in 3 weeks to assess and then regularly
If you have any other question e mail us
Q-28 How much time does it take for the botulin to start acting?
Ans – Typically it starts in 2 weeks -3 weeks but in younger children this starts earlier may be in a week If you have any other question e mail us at
If you have any other question e mail us
If you have any other question e mail us